








What is a Cataract?
To fully understand your cataract surgery and lens choices, it is important to start at the beginning and refresh your knowledge about how the eye works.
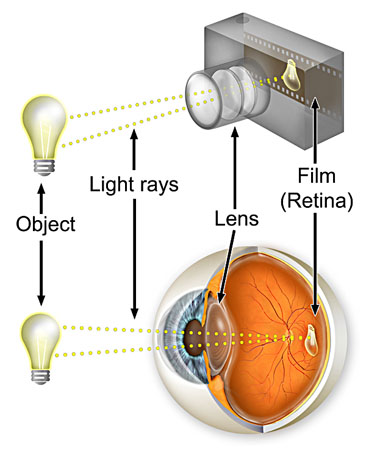
The eye is very much like a camera. The cornea is at the front, rather like an outer lens of a camera with the eyelids as the lens cap. Then comes the iris and pupil that adjust how much light enters the eye. Behind the iris is the focusing lens that directs the rays of light onto the retina. As we age two things happen. Firstly during middle age the lens in our eye stiffens and no longer has the ability to zoom in, and we consequently need reading glasses. Secondly as we age further, the lens stiffens further and starts to become gradually more and more cloudy. This clouding is the cataract. Cataract formation is a normal feature of ageing.
What are the symptoms of cataract?
As cataracts progress there is usually a slow increase in their symptoms. One of the first symptoms is glare, particularly evident from oncoming headlights when driving at night. This glare is caused by the cataract scattering the light entering the eye to the sensitive peripheral retina. The cataract can then cause the lens to swell causing a rapid change in your spectacle prescription, leading to more frequent visits to your optician. The lens yellows, affecting your perception of colours and causing you to need brighter light with which to read. In the final stages the cataract starts to affect your visual acuity directly, reducing your ability to read smaller print and threatening your ability to drive. At this stage patients describe their vision as cloudy, fuzzy, filmy or foggy. The cataract can also cause ghosting with the perception of double vision.


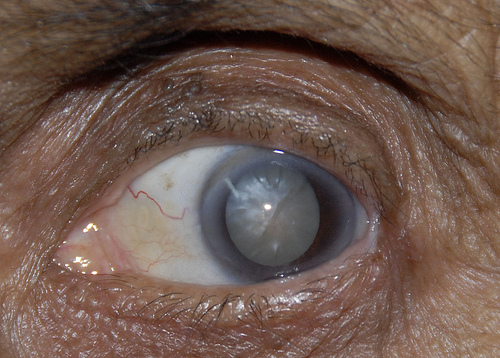
Your optician or GP will normally detect your cataract. They will then refer you to your eye surgeon. Your surgeon would then also confirm the presence of the cataract with microscopic examination in clinic and exclude any other cause for your symptoms. The photo below shows an advanced white cataract.
When is the cataract ready for surgery?
Once your cataract starts to affect your vision it will slowly progress. The timing of surgery varies from individual to individual and depends on lifestyle and activity. Essentially surgery is advised once the symptoms are severe enough to be worth the risk. For someone who drives at night this could be much sooner than for a non-driver.
What are The Risks of Cataract Surgery
Modern cataract surgery is one of the safest and most effective of all operations. No surgery is totally without risk however, and it is important for any patient to understand what can go wrong such that they can make an informed decision to have the surgery. I have summarised the risks and their comparative frequency below. Some of the complications are treatable and should not affect your end result. Other complications are more serious and can damage your vision. Taking all the risks into account the overall chance of your vision being made significantly worse by cataract surgery is about 1 in 1000.
Infection 1:3000
If any bacteria enter the eye at the time of surgery this can lead to an intra-ocular infection. While often treatable, the infection can still sometimes damage the vision. The rate of infection is minimised with strict sterile technique at the time of surgery.
Haemorrhage 1:3000
The tiny blood vessels in the retina can bleed at the time of surgery. This can lead to scarring of the retina and a reduction in your vision. If you are diabetic, it is very important to make sure your retina is fully treated prior to any cataract surgery.
Cystoid Macular Oedema 1:40
The retina can swell up due to the surgery. This can reduce your vision. You may need to take additional drops for a longer period. The condition usually improves over some weeks to months, if it does not resolve your central vision can remain blurred.
Posterior Capsule Rupture 1:50
If the lens capsule is ruptured at the time of surgery it will be difficult to fit your intra-ocular lens. In some circumstances the lens can be placed on the rim of the capsule, in some circumstances the lens can be clipped to your iris and in some circumstances the lens may need to be placed in front of the iris. While the result can still be perfect the surgery will have been more complex, your recovery may be delayed and there is a greater risk of the lens de-centring with a worse visual outcome.
Dropped Nucleus 1:500
If the cataract lens slides through a ruptured posterior capsule into the vitreous (the jelly that fills the main cavity of the eye) then you will need secondary surgery by a vitreo-retinal specialist to remove the cataract. The end result can still be perfect but with the same problems of lens fixation as for any ruptured capsule and with the additional risks of the extra surgery.
Retinal Detachment 1:500
There is an increased risk of retinal detachment for the months following cataract surgery. This risk is greater for patients with myopia (short sight).
Intra-ocular Lens Errors 1:40
The artificial lens placed into your eye is chosen based on pre-operative measurements. Sometimes the lens does not give the expected result and as a result your eye ends up either long or short sighted. If the outcome is significant there are a number of options. The lens can be removed and replaced. A secondary intra-ocular lens can be placed over the lens to correct the refractive error. The cornea can be treated with laser surgery or you could wear either contact lenses or glasses.
Posterior Capsular Opacification 1:10
The outer layer of your old lens is kept to act as a carrier bag for your new lens. This layer can itself thicken. This typically occurs one to two years later and gives the same symptoms as the original cataract. The treatment is straightforward and involves cutting a hole in this layer with a laser. As the treatment is very simple and effective we do not really consider this a risk of cataract surgery, rather more of a nuisance which we are continuing to minimise with modern lens design.